Why Your Knee Hurts After a Sports Injury
If you’ve ever heard a loud pop in your knee during a quick turn or landing, you know how terrifying it feels. That sharp pain, swelling that comes within hours, and the feeling that your knee might give out - these aren’t just minor bruises. They’re signs of a serious knee injury. Two of the most common culprits are tears in the anterior cruciate ligament (ACL) and the meniscus. They both cause knee pain, but they’re completely different injuries with different treatments, recovery times, and long-term risks.
Most people assume if your knee is swollen and painful after a game, you need surgery. But that’s not always true. In fact, more than half of meniscus tears can be treated without an operation. Meanwhile, if you’re under 40 and active, an ACL tear almost always means surgery. Knowing the difference isn’t just about medical facts - it’s about making the right choice for your body and your life.
What Exactly Is the ACL and Meniscus?
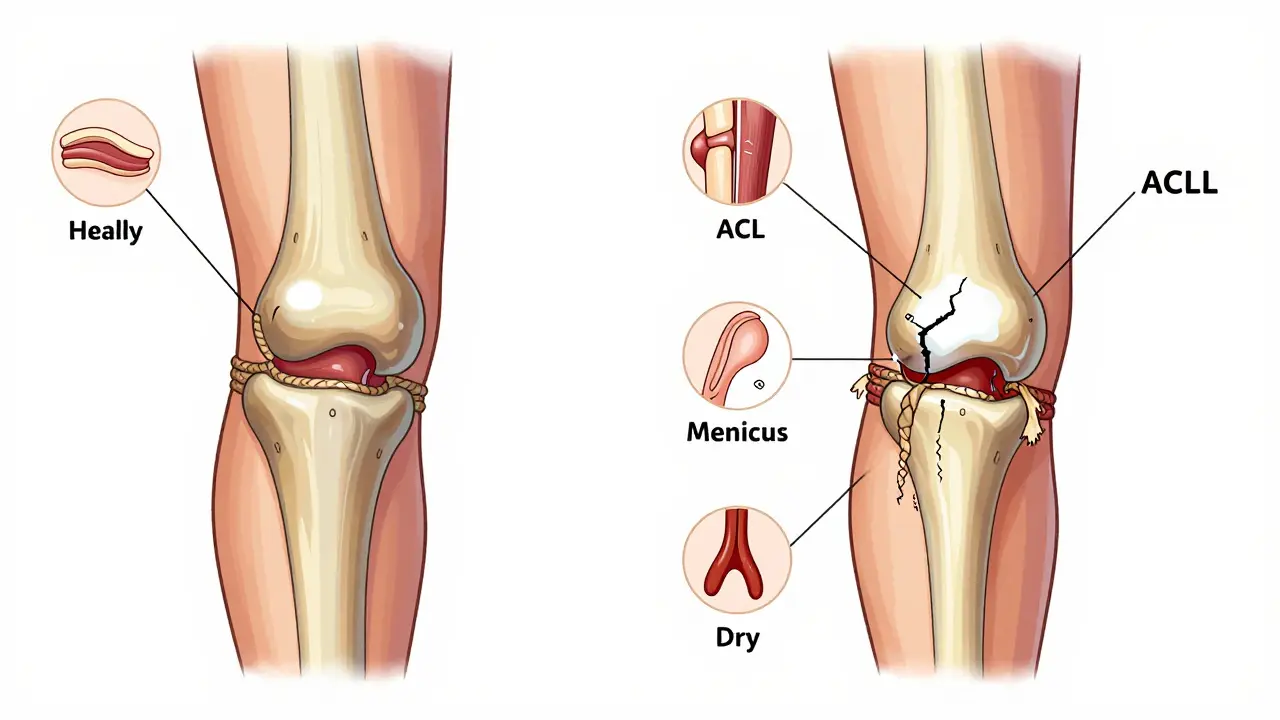
The ACL is a strong band of tissue that runs diagonally in the middle of your knee. Its job? To stop your shinbone from sliding too far forward and to help control twisting motions. Think of it like the main anchor holding your knee steady during cuts, jumps, and sudden stops. It’s about 32mm long and can handle up to 2,160 newtons of force - that’s like holding a small car.
The meniscus, on the other hand, is made of two C-shaped pieces of cartilage - one on the inside (medial) and one on the outside (lateral) of your knee. These act like shock absorbers. They spread out the pressure between your thigh bone and shin bone, protecting the joint surface. About 70% of the meniscus is made of collagen, and it’s mostly water. But here’s the catch: the outer edge has blood flow (the "red zone"), so it can heal. The inner part doesn’t - that’s the "white zone." If a tear happens there, your body can’t fix it on its own.
How Do You Know Which One Is Torn?
The symptoms might sound similar, but the details tell the real story.
ACL tears usually happen without contact - you plant your foot, twist, and your knee gives way. About 90% of people hear a pop. Swelling hits fast - within two hours in 85% of cases. You might feel your knee wobbling or locking when you try to walk. A simple test called the pivot shift test, done by a doctor, can detect this instability with 94% accuracy.
Meniscus tears often come from a twist or squat, especially if you’re older or have worn-down cartilage. The pain is usually focused along the joint line - you can point right to it. Instead of immediate swelling, it often takes 6 to 24 hours. The big red flag? Catching, locking, or your knee getting stuck. If you can’t fully straighten your leg, it’s likely a bucket-handle tear. Meniscus injuries don’t usually make your knee feel unstable like an ACL tear does.
Surgery: When Is It Really Necessary?
Here’s where things get confusing. For ACL injuries, the answer is usually yes - if you’re young and active. Studies show that 95% of people under 40 who play sports like soccer, basketball, or even weekend tennis will need ACL reconstruction. Why? Because without it, your knee will keep giving out. That’s not just annoying - it’s dangerous. Each time your knee buckles, you risk more damage to the meniscus and cartilage, leading to early arthritis.
But for meniscus tears? Only 30 to 40% need surgery. The rest improve with rest, physical therapy, and time. If your tear is small, in the outer red zone, and you’re not locking up, doctors will often recommend at least 6 to 8 weeks of rehab before even thinking about surgery. Many people, especially over 40, do just fine without an operation.
But if you have a large, displaced tear - like a bucket-handle - or you’re young and active with mechanical symptoms, repair or removal becomes necessary. A repair is better than a removal because it preserves your natural cartilage. But it’s not always possible. If the tear is in the white zone, it won’t heal, so surgeons have to trim the damaged part out (a meniscectomy).
Types of Surgeries and What They Mean for Recovery
ACL reconstruction isn’t just "fixing" the ligament. It’s replacing it. Surgeons use your own tissue - either the hamstring tendons or the middle third of your patellar tendon. Hamstring grafts are more common now because they cause less front-of-knee pain. Bone-patellar-tendon-bone grafts are stronger, but they’re harder on the kneecap. Allografts (donor tissue) are faster to recover from initially, but they have a much higher failure rate in young athletes - up to 22% compared to 7.7% with your own tissue.
Meniscus repair uses tiny sutures to stitch the torn edges together. It’s trickier than ACL surgery. The tear has to be in the right spot (red zone), and you have to get it done within 8 weeks for the best chance of healing. After repair, you’re in a brace for 6 weeks and can’t put full weight on the leg. Return to sports? 5 to 6 months. That’s long. But it’s worth it - keeping your meniscus cuts your risk of arthritis by half.
Meniscectomy, the removal of the torn part, is faster. You can walk the same day. Return to light activity? 2 to 4 weeks. Full recovery? 6 to 8 weeks. But here’s the trade-off: every 10% of meniscus you remove increases your risk of osteoarthritis by 14%. That’s not a small number. It means if you lose half your meniscus, your risk of arthritis doubles.
Cost, Success Rates, and Real Patient Stories
ACL reconstruction costs between $15,000 and $25,000. Meniscus repair runs $9,000 to $18,000. Meniscectomy is cheaper - $6,000 to $12,000. But the real cost isn’t just the bill. It’s the time. ACL rehab takes 9 months before you can safely return to pivoting sports. Skip that timeline? Your chance of re-tearing the ACL jumps from 5% to 22%.
Patients who get ACL reconstruction report 82-92% satisfaction at two years. But 20-30% develop arthritis within a decade. Meniscectomy has 85-90% short-term success, but 67% of patients report some level of ongoing discomfort after six months. One Reddit user shared: "I had a meniscus repair. First 6 weeks in a brace, couldn’t bend past 90 degrees. Now I’ve got a 20-degree permanent loss in extension. I can’t fully straighten my leg." Another said: "After ACL surgery, my quad muscle was 15% smaller than the other leg at 12 months. I still feel weak."
Surgeons with more experience - those who’ve done 50+ ACL reconstructions - have better outcomes. The same goes for meniscus repairs. If your surgeon has done fewer than 30 repairs, ask about their success rate.
What Happens If You Wait Too Long?
Delaying treatment can cost you options. For meniscus tears, waiting more than 3 months reduces your chance of repair by 60%. Why? The torn edge gets frayed, the tissue weakens, and what could’ve been stitched back together now has to be cut out. By then, your chances of needing a meniscectomy jump from 35% to 85%.
For ACL injuries, waiting isn’t as urgent - but it’s risky. Every time your knee gives out, you scrape more cartilage off your bones. That damage is permanent. Studies show that people who wait more than 6 months to get ACL surgery have a 50% higher chance of developing a second meniscus tear.
Can You Avoid Surgery Altogether?
Yes - but only if you’re realistic about your goals.
If you’re over 40, don’t play high-impact sports, and your knee doesn’t lock or give way, you can often manage both injuries without surgery. Physical therapy focused on quad and hamstring strength, balance training, and activity modification can get you back to walking, swimming, cycling, and even golfing without pain.
For younger people, non-surgical treatment for ACL tears is usually a dead end. You might get by for a while, but if you want to play soccer, ski, or even do intense gym workouts, you’ll likely end up with more damage. The exception? Some older adults with low-demand lifestyles who choose to avoid surgery. But they must accept that they’ll never return to cutting sports.

What’s New in Treatment?
There’s exciting progress. Surgeons are now using biologic boosters like platelet-rich plasma (PRP) during meniscus repairs. One 2025 study showed PRP improved healing rates in the red-white zone by 25%. Meniscus transplants - using donor cartilage - are becoming more common for people who’ve lost a large portion of their meniscus. Five-year success rates are around 85%.
Prehab is also making a big difference. Patients who do 6 weeks of strengthening before ACL surgery cut their post-op muscle loss in half. Instead of losing 22% of quad strength, they lose only 8%. That’s huge for recovery speed.
And prevention? Programs like FIFA 11+ - a 20-minute warm-up routine - have cut ACL injuries by half in young athletes. It’s not magic. It’s balance drills, strengthening, and proper landing technique. More schools and clubs are starting to use it.
Final Decision: What Should You Do?
Here’s a simple guide:
- If you’re under 40 and active - and you heard a pop with immediate swelling - get an MRI. ACL reconstruction is likely your best path.
- If your knee locks or catches - and you’re under 50 - see a specialist within 2 weeks. You might still be able to repair the meniscus.
- If you’re over 50 and have mild pain without locking - try physical therapy first. Surgery won’t fix arthritis.
- If you’re told you need surgery - ask: Is this a repair or a removal? What’s my graft option? How many of these have you done?
Your knee isn’t just a joint. It’s your mobility, your independence, your ability to move without pain. The right decision now can keep you active for decades. The wrong one? It might lead to a knee replacement before you turn 50.
Frequently Asked Questions
Can a meniscus tear heal on its own?
Only if it’s in the outer third of the meniscus, where there’s blood flow - called the red zone. Tears in the inner two-thirds (white zone) won’t heal without help. Even red-zone tears need time and protection. Most doctors recommend 6 to 8 weeks of rest and physical therapy before considering surgery.
How long does ACL recovery really take?
It’s not 6 months. Most athletes need 9 months, and many need up to 12. Returning too early - before 9 months - increases your risk of re-tearing the ACL by 18%. You need to pass strength tests (like single-leg hop symmetry over 90%), balance drills, and sport-specific movements before you’re cleared. Skipping steps leads to more injuries down the road.
Is an allograft (donor tissue) a good option for ACL reconstruction?
For people over 40 who don’t play high-impact sports, maybe. But for athletes under 25, it’s risky. Allografts have a 22% failure rate in young, active patients compared to 7.7% with your own tissue. They heal faster at first, but they’re more likely to stretch or break over time. Most surgeons avoid allografts for teens and young adults.
Will I get arthritis after ACL or meniscus surgery?
There’s a good chance - especially if you’ve had a meniscectomy. Removing even a small part of the meniscus increases your arthritis risk by 14% per 10% removed. After ACL injury, 20-30% develop arthritis within 10 years, even with surgery. The best way to delay it? Keep your knee strong, maintain a healthy weight, and avoid high-impact sports long-term.
Can I still run or play sports after meniscus repair?
Yes - if the repair heals. But you need patience. Most people can’t run until 4 to 5 months after surgery, and cutting sports like basketball or soccer usually take 6 months. You’ll need to pass strength and movement tests. Rushing it risks re-tearing the meniscus. But if it works, you’ll have better long-term joint health than if you’d had the meniscus removed.
What’s the biggest mistake people make after knee surgery?
Skipping physical therapy or quitting too early. Many patients feel better after 6 weeks and think they’re done. But muscle weakness, poor balance, and stiff joints linger. That’s when re-injury happens. The most successful patients stick with therapy for the full timeline - even when it’s boring or painful.
Next Steps: What to Do Right Now
If you’re dealing with knee pain after an injury:
- Stop high-impact activity immediately. Don’t push through the pain.
- See a sports medicine specialist within 2 weeks. Get an MRI - X-rays won’t show soft tissue damage.
- Ask your doctor: Is this a repairable tear? Is surgery truly necessary?
- If surgery is recommended, ask about graft type (for ACL) and whether it’s repair or removal (for meniscus).
- Start physical therapy now - even before surgery. Strengthening your quads cuts recovery time and improves outcomes.
Your knee doesn’t need to be fixed overnight. It needs the right plan - and the patience to follow it. The goal isn’t just to walk again. It’s to move without pain for the rest of your life.





15 Comments