DOAC Dose Calculator for Renal Impairment
Why DOACs Can Be Dangerous in Kidney Problems
Direct Oral Anticoagulants, or DOACs, are meant to be simpler than warfarin. No weekly blood tests. No strict diet rules. Just take your pill and go. But if your kidneys aren’t working well, that simplicity turns risky. About 1 in 4 people with atrial fibrillation also have kidney disease. That’s not rare. It’s common. And if you don’t adjust the dose correctly, you could bleed internally-or form a deadly clot.
DOACs like apixaban, rivaroxaban, dabigatran, and edoxaban leave your body mostly through your kidneys. When kidneys slow down, the drug builds up. Too much? Bleeding risk spikes. Too little? Stroke risk jumps. The stakes are high. A single wrong dose can land someone in the ER-or worse.
How to Measure Kidney Function for DOACs (It’s Not What You Think)
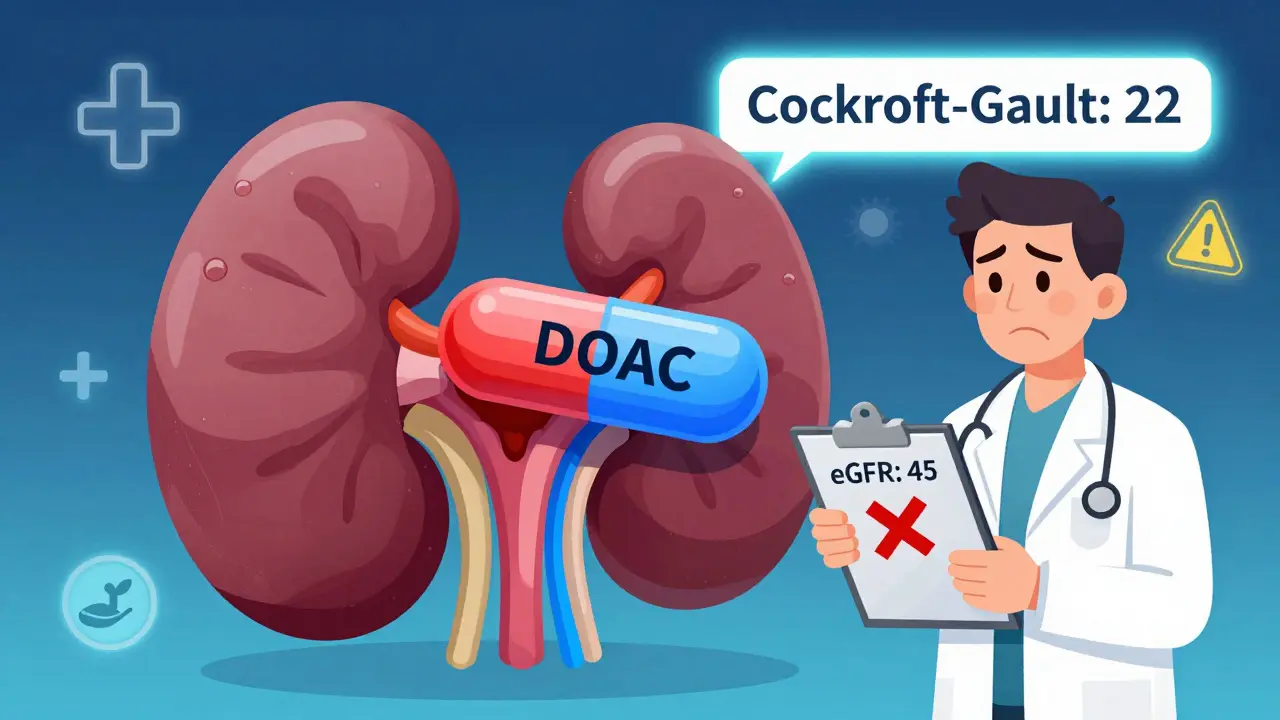
You’ve probably heard of eGFR. Doctors use it all the time. But for DOACs? It’s not good enough. The FDA, the American Heart Association, and kidney experts all agree: use the Cockcroft-Gault formula. Not eGFR. Not serum creatinine alone. The Cockcroft-Gault equation, which factors in age, weight, sex, and creatinine, is the only accepted method.
Why? Because eGFR doesn’t account for low muscle mass. Elderly patients, frail people, or those with low body weight often have misleadingly low creatinine levels. Their eGFR looks okay. But their real kidney clearance? It’s terrible. That’s where Cockcroft-Gault catches the error. A 78-year-old woman weighing 50 kg might have an eGFR of 45 mL/min-but her actual creatinine clearance could be 22 mL/min. Give her full-dose rivaroxaban? That’s a recipe for bleeding.
Apixaban: The Safest Option for Kidney Patients
Among all DOACs, apixaban stands out. It’s the least dependent on kidney function. About 25% of apixaban is cleared by the kidneys. The rest is broken down by the liver. That’s why it’s the only DOAC with data showing safety even in patients on dialysis.
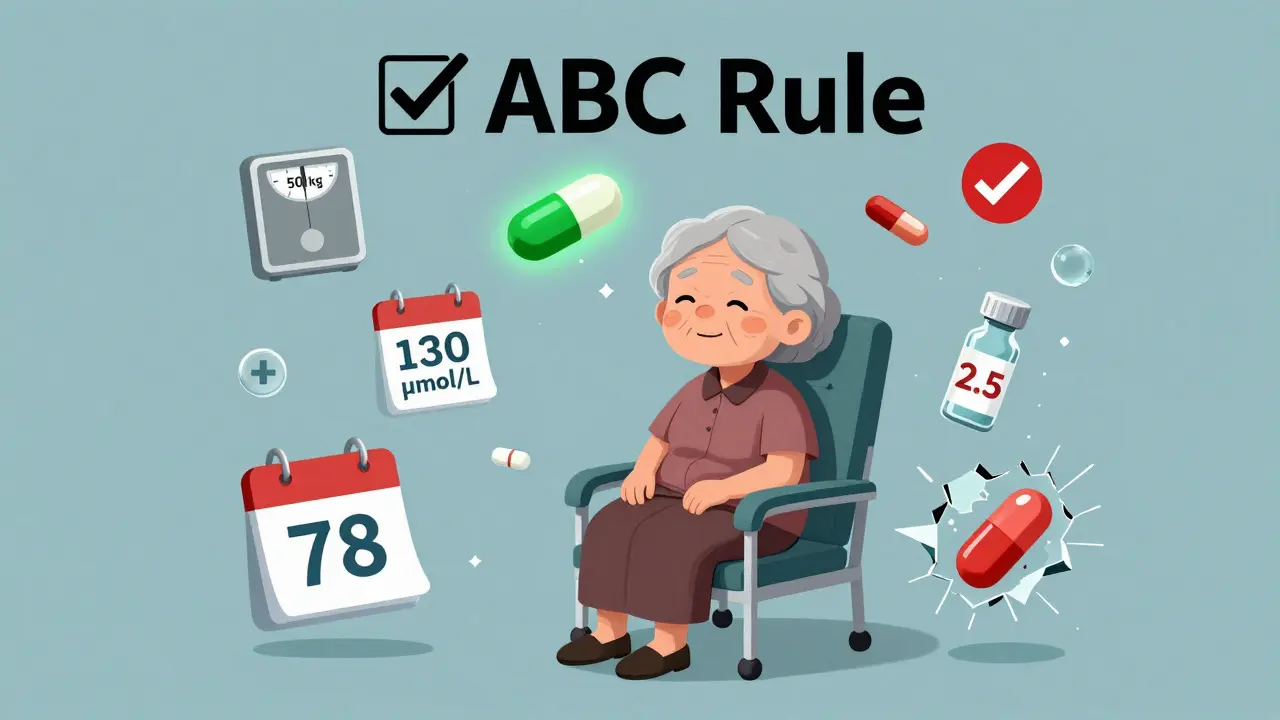
The standard dose is 5 mg twice daily. But you drop to 2.5 mg twice daily if the patient meets any two of these three criteria: age 80 or older, body weight 60 kg or less, or serum creatinine 133 μmol/L or higher (1.5 mg/dL). That’s it. No need to memorize CrCl ranges. Just check the box.
Studies show apixaban causes less major bleeding than warfarin in patients with end-stage kidney disease. One real-world study tracked 127 dialysis patients on apixaban 2.5 mg twice daily. Major bleeding happened in just 1.8% per year. In their warfarin group? 3.7%. That’s a 50% drop. Apixaban isn’t perfect-but it’s the best option we have for advanced kidney disease.
Rivaroxaban, Dabigatran, Edoxaban: When to Avoid or Reduce
Rivaroxaban? Don’t use it if CrCl is below 15 mL/min. Period. Even 15-29 mL/min? Use with extreme caution. Most guidelines say avoid entirely in dialysis patients.
Dabigatran is even trickier. You can use 75 mg twice daily if CrCl is between 15 and 30 mL/min. But below 15? Absolutely contraindicated. It’s almost entirely cleared by the kidneys. In one case series, a patient on full-dose dabigatran with CrCl of 12 mL/min bled into the gut and died within 48 hours.
Edoxaban? Reduce to 30 mg once daily if CrCl is 15-50 mL/min. Below 15? Don’t use. The ENGAGE AF trial showed edoxaban lost effectiveness in patients with poor kidney function. It didn’t protect against stroke as well as in healthy kidneys.
Bottom line: apixaban is the only DOAC you can confidently use in severe kidney disease. The others? Only if CrCl is above 30 mL/min-and even then, check the dose.
Common Mistakes Doctors and Pharmacists Make
A 2022 study in JAMA Internal Medicine found that nearly 4 out of 10 DOAC prescriptions in kidney patients were dosed wrong. Here’s how it happens:
- Using eGFR instead of Cockcroft-Gault: The most frequent error. Leads to underestimating risk.
- Forgetting the ABC rule for apixaban: Age, weight, creatinine. Two out of three? Reduce the dose. Don’t wait for CrCl to drop below 30.
- Prescribing rivaroxaban for dialysis patients: Still happens. Even though guidelines say no.
- Not rechecking kidney function: Kidneys can decline fast. A patient with CrCl of 45 in January might be at 22 by June. Yet the dose stays the same.
Pharmacists report that elderly patients with low muscle mass are especially hard to assess. Their creatinine looks normal. Their weight is low. Their age is high. But they’re not getting enough drug. Or they’re getting too much. It’s a tightrope.
What to Do If You’re on a DOAC and Have Kidney Disease
If you’re taking a DOAC and you know you have kidney problems, here’s what to ask your doctor:
- What’s my actual creatinine clearance? Not eGFR. Cockcroft-Gault.
- Am I on the right dose based on my age, weight, and creatinine?
- Have you checked my kidney function in the last 3 months?
- Is apixaban the best option for me-or should we switch?
- What signs of bleeding should I watch for? (Black stools, dizziness, unusual bruising, headaches)
Don’t assume your doctor knows. Many don’t. A 2022 study of hospitalists showed it takes 3-6 months of experience to get DOAC dosing right. If you’re on dialysis, ask specifically about apixaban 2.5 mg twice daily. That’s the dose with the most real-world evidence.
The Future: What’s Coming in 2025 and Beyond
Right now, we’re flying blind in some areas. There’s no solid data on whether DOACs work better than warfarin in dialysis patients. That’s why the RENAL-AF trial is so important. It’s comparing apixaban to adjusted warfarin in patients with CrCl under 30 mL/min. Results are expected in 2025.
Meanwhile, apixaban is already being used off-label in dialysis patients-and working better than expected. The global DOAC market is growing fast, and more doctors are choosing apixaban for kidney patients, even when labels don’t fully support it.
By 2026, guidelines will likely change. We’ll have clearer rules for every stage of kidney disease. But until then, stick to the evidence: use apixaban at reduced dose when needed. Avoid rivaroxaban and dabigatran in severe disease. And always, always use Cockcroft-Gault.
Final Takeaway: Don’t Guess. Calculate.
DOACs are powerful. They save lives. But they can kill if dosed wrong in kidney disease. The key isn’t memorizing charts. It’s asking the right questions: What’s my CrCl? Am I on the right dose? Is this the safest drug for me?
If you have kidney disease and need a blood thinner, apixaban at 2.5 mg twice daily is your safest bet. For mild to moderate kidney problems, any DOAC can work-if the dose is correct. But never skip the calculation. Never assume. And never use eGFR to guide your dose. Your life depends on the numbers being right.





8 Comments
Apixaban being the least renal-dependent makes total sense. I’ve seen so many elderly patients on rivaroxaban with eGFR of 40 and no dose adjustment-total accident waiting to happen. The Cockcroft-Gault point is spot on. I wish more hospitals forced it into their EHR defaults instead of letting eGFR autopilot everything.
It is imperative to underscore that the utilization of estimated glomerular filtration rate (eGFR) for direct oral anticoagulant (DOAC) dosing in the context of chronic kidney disease constitutes a clinically significant deviation from evidence-based guidelines. The Cockcroft-Gault equation remains the gold standard due to its incorporation of weight, age, and sex-parameters that are demonstrably absent from eGFR calculations. Failure to adhere to this standard exposes patients to unacceptable hemorrhagic risk.
Oh wow, a whole post about not killing people with blood thinners. Who knew? In the UK we’ve been doing this since 2012. Guess we’re just too advanced over here for your 2024 medical education.
Real talk-my grandma was on apixaban 2.5mg twice and her creatinine was 1.4. Doc used eGFR and said she was fine. I pulled up Cockcroft-Gault myself. CrCl was 21. We switched. She’s still alive. Never trust eGFR alone.
apixaban for dialysis patients is the only thing that makes sense honestly i’ve seen too many people bleed out from wrong doses
you know what’s funny? we spend billions on fancy drugs but forget to calculate kidney function properly. it’s like buying a supercar and then ignoring the fuel gauge. the body doesn’t care about guidelines, it cares about what’s actually in the blood. apixaban’s liver clearance is a gift. maybe we should stop pretending all kidneys work the same.
This is exactly why we need mandatory continuing medical education on anticoagulant dosing in renal impairment. In India, many physicians still rely on serum creatinine alone. We’ve had preventable deaths in tertiary centers because of this. Apixaban at 2.5 mg BID in dialysis isn’t off-label-it’s lifesaving. We must standardize this. Let’s train our pharmacists, our residents, our nurses. Knowledge is not optional. It’s survival.
I appreciate the clarity here. As a clinician in Nigeria, I’ve seen patients come in with severe renal impairment on full-dose dabigatran because their local pharmacy didn’t question the prescription. We don’t always have access to Cockcroft-Gault calculators, but we do have pen and paper. I’ve started printing simple charts for my team. One page. Age, weight, creatinine. Multiply. Divide. It’s old school, but it saves lives. Thank you for the reminder that sometimes the simplest tools are the most powerful.