When chronic pain won’t go away, pills and physical therapy often aren’t enough. That’s where nerve blocks and radiofrequency ablation (RFA) a minimally invasive procedure that uses heat to disrupt pain-signaling nerves come in. These aren’t surgeries. They’re precise, outpatient procedures designed to stop pain signals before they reach your brain. And for many people with persistent back, knee, or neck pain, they offer real relief - without opioids or long recovery times.
How Nerve Blocks Work (and Why They’re Just the First Step)
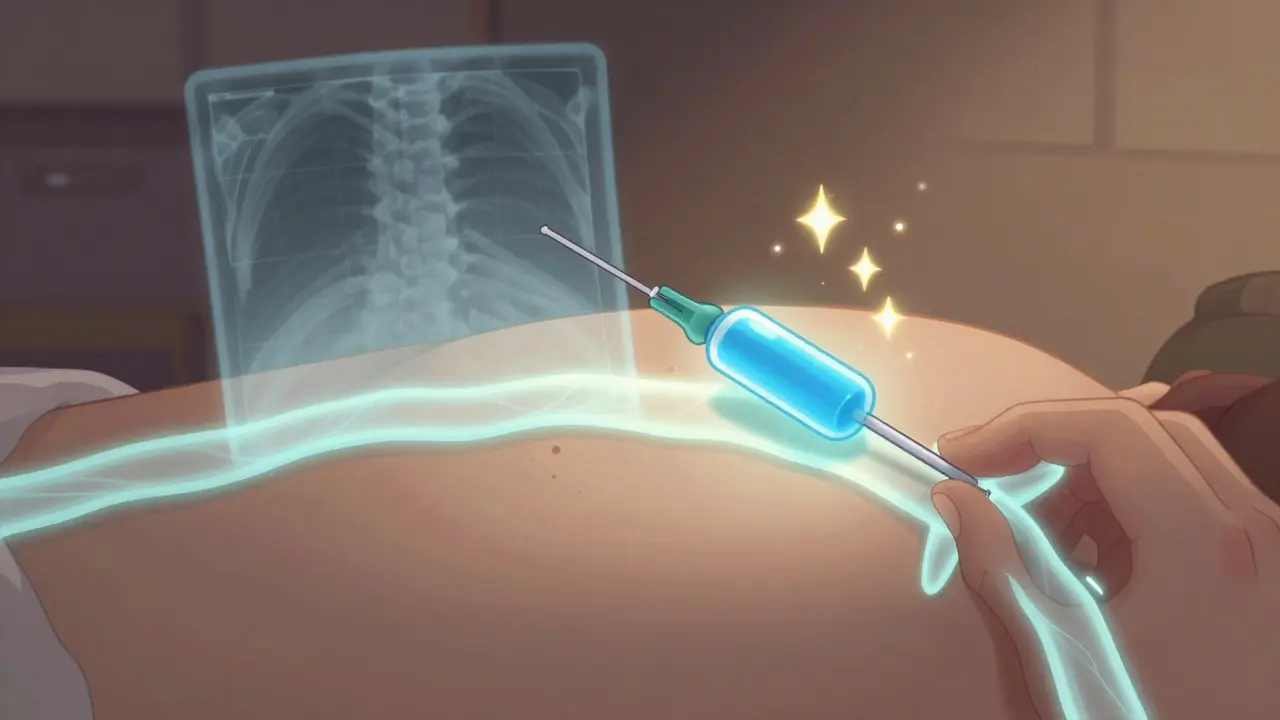
Nerve blocks are simple in concept: inject a numbing medicine - usually a local anesthetic like lidocaine - near a nerve that’s sending pain signals. Think of it like flipping a temporary switch. The pain disappears for a few hours, sometimes up to a few weeks. But here’s the catch: the real purpose of a nerve block isn’t to treat pain long-term. It’s to diagnose it.
Doctors use nerve blocks to answer one critical question: Is this specific nerve the source of your pain? If you get 80% or more pain relief after the injection, it’s a strong sign that nerve is responsible. If not? Then the problem is elsewhere. This step is non-negotiable. Skipping it leads to failed RFA procedures. Studies show up to 30% of RFA attempts fail because the wrong nerve was targeted in the first place.
Common targets include the medial branches of the spine (for low back pain), the genicular nerves around the knee (for osteoarthritis), and the occipital nerves at the base of the skull (for headaches). Each block takes less than 15 minutes, done with live X-ray guidance (fluoroscopy) to make sure the needle goes exactly where it should.
What Is Radiofrequency Ablation (RFA)?
RFA is what happens when a nerve block works - but you need something that lasts longer than a few days.
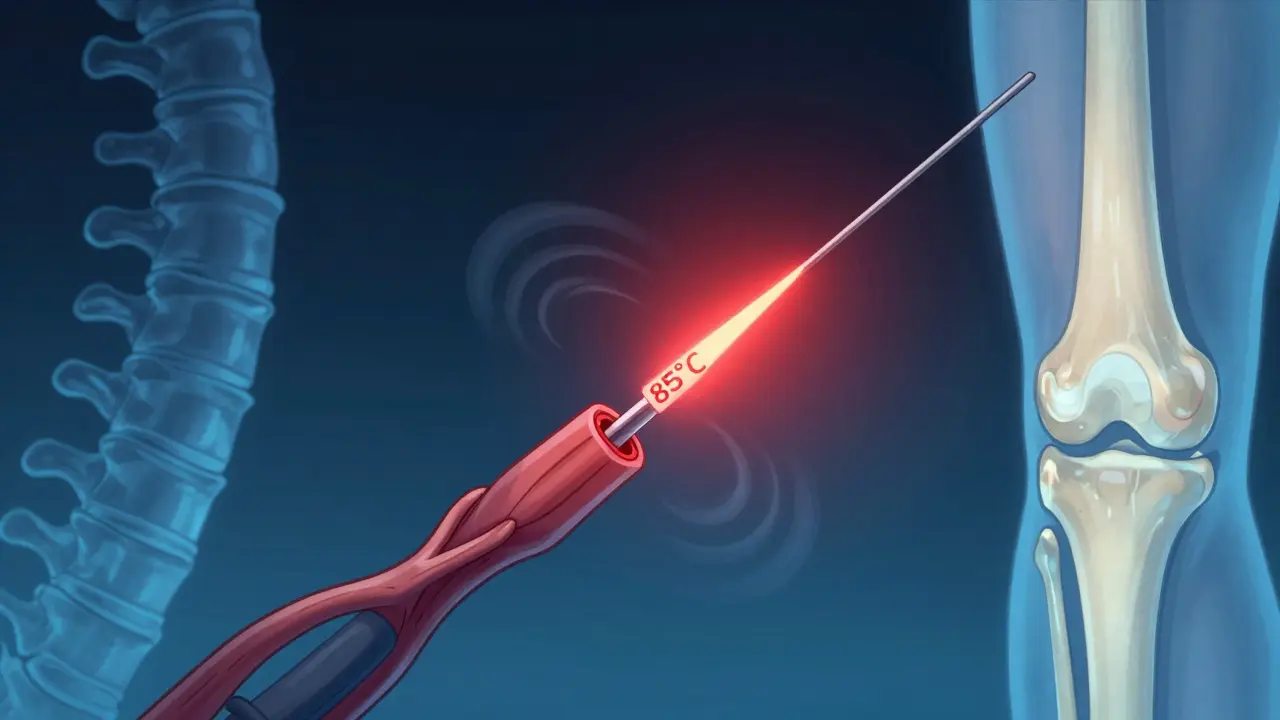
Instead of injecting medicine, RFA uses a thin needle to deliver controlled heat - between 80°C and 90°C - directly to the nerve. This heat creates a tiny lesion, essentially scarring the nerve just enough to stop it from sending pain signals. The nerve doesn’t die. It regenerates slowly over time, which is why relief lasts 6 to 24 months, not forever.
Modern RFA uses 22-gauge needles with 5mm exposed tips. Before heating, the doctor tests placement by sending a tiny electrical current through the needle. If you feel tingling (not pain), the needle is near the right nerve. Then, they turn on the radiofrequency generator. The whole procedure takes 20 to 45 minutes, depending on how many nerves are treated. You’re awake, lightly sedated, and go home the same day.
There’s also a variation called pulsed radiofrequency (PRF) a non-thermal method that modulates nerve activity without burning tissue. Instead of heat, it uses short bursts of high-voltage energy. PRF is less invasive and may be used when nerves are too close to muscles or other sensitive structures. It’s not as long-lasting as traditional RFA, but it’s a good option for some patients.
RFA vs. Nerve Blocks: The Real Difference
People often confuse the two. Here’s how they actually compare:
| Feature | Nerve Block | Radiofrequency Ablation (RFA) |
|---|---|---|
| Primary Purpose | Diagnosis and short-term relief | Long-term pain management |
| Duration of Relief | Hours to weeks | 6 to 24 months |
| Method | Injection of anesthetic or steroid | Heat lesion created by radiofrequency energy |
| Procedure Time | 10-15 minutes | 20-45 minutes |
| Recovery Time | Same day | Same day, mild soreness for 3-7 days |
| Success Rate (in Proper Candidates) | 30-50% beyond immediate relief | 70-85% with confirmed diagnostic block |
Think of it this way: a nerve block is like turning off a light switch for a few hours. RFA is like rewiring the circuit so the switch doesn’t work for a year or two. You still need the switch test first.
Who Benefits Most From RFA?
RFA isn’t for everyone. It’s best for people who:
- Have chronic pain that hasn’t improved with physical therapy, NSAIDs, or steroid injections
- Got clear, lasting relief (80%+) from a diagnostic nerve block
- Are between 45 and 65 years old - this group shows the highest success rates
- Want to avoid surgery or reduce opioid use
The strongest evidence is for:
- Facet joint pain (lower back or neck pain from arthritic joints): 70-80% success rate
- Knee osteoarthritis: Cooled RFA helps 65% of patients maintain relief at 6 months
- Sacroiliac joint pain: 70% success at 6 months
- Occipital neuralgia (chronic headaches): Significant reduction in frequency and intensity
It’s not a cure. If you have severe arthritis, RFA won’t fix the joint damage. But it can stop the pain signals, letting you move, sleep, and live better.
What to Expect Before, During, and After
Before: You’ll have a diagnostic nerve block first. If it works, you schedule RFA within a few weeks. No fasting needed, but you’ll need someone to drive you home.
During: You’re awake but relaxed. The area is numbed. The needle goes in with real-time X-ray guidance. You might feel pressure, but not sharp pain. The heat feels like warmth, sometimes a brief pinch. You’ll be asked to report any sensations - this helps the doctor confirm placement.
After: Expect mild soreness at the injection site for 3-7 days. It’s normal. Full pain relief usually takes 2-4 weeks as the nerve heals around the lesion. Most people return to work in 1-2 days. No heavy lifting for a week. You can resume walking, light chores, and driving right away.
Side effects are rare. Less than 5% get temporary nerve inflammation. Permanent nerve damage? Extremely rare - less than 1 in 1,000 cases - when done by trained specialists.
Why RFA Is Changing Pain Management
In 2023, about 350,000 RFA procedures were done in the U.S. alone. That number is growing 15% each year. Why? Because it works - and it’s a smart alternative to opioids.
CMS data shows Medicare patients who got RFA cut their long-term opioid use by 22%. That’s huge. It’s also cheaper than surgery. A single RFA costs $3,000-$5,000. A spinal fusion? $50,000+. Even spinal cord stimulators - which need implants - cost 10 times more.
Technology is improving too. cooled RFA uses internal cooling to create larger, more effective lesions is now standard for knee and spine treatments. The FDA approved pulsed-field ablation in 2022 - a non-thermal option that may reduce recovery time even further.
Experts like the American Society of Anesthesiologists now recommend RFA as a standard second-line treatment after physical therapy and injections fail - before you even consider surgery.
When RFA Doesn’t Work - And Why
It’s not magic. Failure usually happens because:
- The diagnostic nerve block wasn’t done right - or wasn’t done at all
- The pain isn’t nerve-related (e.g., muscle strain, systemic inflammation)
- The nerve regenerates faster than expected (some people heal in 4-6 months)
- The procedure was done by someone without proper training
That’s why experience matters. The American Society of Regional Anesthesia recommends at least 50 supervised RFA procedures before a doctor performs them independently. Ask your provider: How many have you done? What’s your success rate?
Is RFA Right for You?
If you’ve tried physical therapy, pain meds, and steroid injections - and still hurt - RFA might be the next step. But don’t jump straight to it. You need:
- A clear diagnosis
- A successful diagnostic nerve block
- A specialist trained in interventional pain management
It’s not a first-line treatment. It’s a smart, targeted tool - used at the right time, it can change your life.
Are nerve blocks and RFA the same thing?
No. Nerve blocks use medicine to temporarily block pain signals. RFA uses heat to disable the nerve for months. Nerve blocks are used to test if RFA will work. You need a successful nerve block before doing RFA.
How long does pain relief last after RFA?
Most people get relief for 6 to 24 months. It depends on the nerve, your body’s healing rate, and the condition being treated. For example, facet joint pain often lasts 12-18 months. Knee pain relief from cooled RFA typically lasts 6 months. The nerve eventually regenerates, and pain may return - but the procedure can be repeated safely.
Is RFA painful?
The procedure itself isn’t painful. The skin is numbed, and you’re given light sedation. You might feel pressure or warmth during the heat phase. Some patients report a brief tingling or muscle twitch - that’s normal and helps the doctor confirm placement. Afterward, mild soreness for a few days is common, but not severe pain.
Can RFA be used for neck pain?
Yes. RFA is commonly used for cervical facet joint pain - a frequent cause of chronic neck pain and headaches. The procedure targets the medial branch nerves in the upper spine. Success rates are similar to lower back RFA: 70-80% for patients who had a positive diagnostic block.
Does RFA damage other nerves or muscles?
No, not when done correctly. The heat is focused only on the targeted nerve. Fluoroscopic imaging and electrical testing ensure the needle is placed precisely. Motor nerves and muscles nearby are preserved because the technique avoids overheating surrounding tissue. Serious complications like paralysis or muscle weakness are extremely rare.
Is RFA covered by insurance?
Yes, most major insurers - including Medicare and private plans - cover RFA when it’s preceded by a successful diagnostic nerve block and used for approved conditions like facet joint pain or knee osteoarthritis. Pre-authorization is usually required. Always check with your provider and insurance before scheduling.
Can I have RFA more than once?
Absolutely. Nerves regenerate over time, so pain can return. RFA can be safely repeated every 6-12 months if needed. Many patients get 2-3 treatments over several years. Each repeat procedure follows the same steps and has similar success rates.
If you’ve been living with chronic pain and feel like you’ve run out of options, RFA might be the bridge you need - between medication and surgery, between suffering and getting your life back.




12 Comments
Man, I wish I knew about nerve blocks before I went through 3 years of steroid injections that did jack. The diagnostic part is genius - it’s not just a treatment, it’s a truth serum for your nervous system. I had lower back pain for ages, thought it was a herniated disc, turned out it was just facet joint inflammation. One block, 90% relief for 3 weeks, RFA after, and now I’m lifting weights again. No opioids, no surgery. Just science.
It is fascinating how this modality operates not as a curative intervention, but as a neuromodulatory intervention - a deliberate, controlled disruption of nociceptive signaling rather than an attempt to reverse structural pathology. The philosophical implication is profound: we are not treating disease, we are attenuating perception. One must ask, if pain is a signal, and we silence the signal, have we not merely obscured the symptom without addressing the cause? Or perhaps, in chronic pain, the signal has become the disease itself.
OMG I’ve been saying this for YEARS. Why do people just pop pills like candy? 😤 This is why America’s in the shitter - everyone wants a quick fix. RFA is the REAL answer. I did it last year. Felt like a tiny zap, then boom - 18 months pain-free. Why are we still letting people waste money on PT? 🤡
I appreciate how this article emphasizes diagnostic precision. Too often, patients are rushed into procedures without confirming the source. I’ve seen friends undergo RFA without a prior block - and it failed. The success rate drops dramatically without that step. It’s not just about the technology - it’s about discipline in diagnosis. That’s what separates competent care from lucky guesses.
Let me guess - this is all funded by Big Med. You know what they don’t tell you? RFA is just a way to keep people coming back for repeat procedures. The nerve regenerates? Perfect. Now they bill you again. And who profits? The clinic. Not you. The FDA approved pulsed-field ablation in 2022? That’s not innovation - that’s rebranding. They’re just selling the same thing with a new name. And don’t get me started on fluoroscopy - radiation exposure adds up. They’re not worried about your long-term health. They’re worried about your insurance card.
In India, access to these procedures is extremely limited. Most people rely on painkillers or traditional therapies. But I’ve read about RFA and find it deeply respectful of the body’s natural healing - it doesn’t destroy, it modulates. The idea that the nerve regenerates slowly, and that relief can be repeated safely, feels almost… spiritual. Like working with biology, not against it. I hope one day these options become available to more people outside the U.S. healthcare bubble.
I find it deeply troubling that this article frames RFA as a 'smart alternative to opioids.' It implies that the opioid crisis was somehow solved by replacing one medical intervention with another. The truth is: chronic pain patients were abandoned by the system, then pushed into pills, then pushed into procedures - all while the root causes - poverty, lack of mental health care, occupational trauma - were ignored. This is not progress. This is damage control dressed up as innovation.
I had RFA on my knee last year and honestly? Best decision ever. I was so skeptical - I thought it was gonna be some shady laser thing. But the doc was super chill, explained everything, even let me watch the screen during the procedure (yes, I saw the nerve lighting up like a Christmas tree 😅). Sore for 4 days, then BAM - no more pain climbing stairs. I’ve been walking 5 miles a day since. My dog’s happy, my knees are happy, I’m happy. If you’ve been stuck in pain hell and tried everything else? Just do the damn block first. Then RFA. You won’t regret it.
Ugh. Another Silicon Valley tech bro solution. We’re not robots. You can’t just zap pain like a bug. What about inflammation? What about muscle imbalances? What about trauma? This is just another way to avoid real rehab. And don’t even get me started on how they charge $5k for this. My cousin got it done in Mexico for $800. Why are we letting American doctors milk this? It’s capitalism, not medicine.
I just had my second RFA last month. First one was 18 months ago. Pain came back - not as bad, but enough to ruin sleep. Did it again. Same doc. Same process. Still 70% relief. I’m 52. I don’t want surgery. I don’t want pills. This is my middle ground. The only thing I wish they told me? That the soreness after is worse than the procedure. But honestly? Worth it. If you’re on the fence - go for the block. If it works, you’ll know.
Just a quick note - if you’re considering RFA, make sure your provider uses cooled radiofrequency for knee treatments. Standard RFA doesn’t create a large enough lesion for genicular nerves. Cooled RFA has a 65%+ success rate at 6 months. Also - no, you don’t need to be 45-65. I’m 38 and it worked great. Age isn’t the barrier - diagnostic accuracy is. Don’t let anyone tell you otherwise.
While the clinical data presented is statistically compelling, one must consider the broader epistemological framework within which this intervention is situated. The assumption that pain is a localized, neuroanatomical phenomenon - and thus amenable to focal ablation - presupposes a Cartesian model of the body. Yet emerging research in neurophenomenology suggests chronic pain is an emergent property of central sensitization, not merely peripheral signaling. To treat the symptom as the disease may be, in the long term, a form of epistemic violence. One must question: are we healing, or merely silencing?